Endoscopic spine surgery (ESS) is an ultra minimally invasive surgical procedure that effectively relieves chronic low back and leg pain.
This state-of-the-art spine surgery utilizes an HD camera attached to an endoscope inserted through a ¼ inch skin incision to the target pain generator in your spine.
The endoscopic orthopedic procedure allows spine surgeons to operate safely, with greater accuracy, and offer patients better outcomes.
The surgeon can observe the spine on an HD monitor and operate through the endoscope using highly specialized micro-instruments like a laser, radiofrequency probe, or graspers.
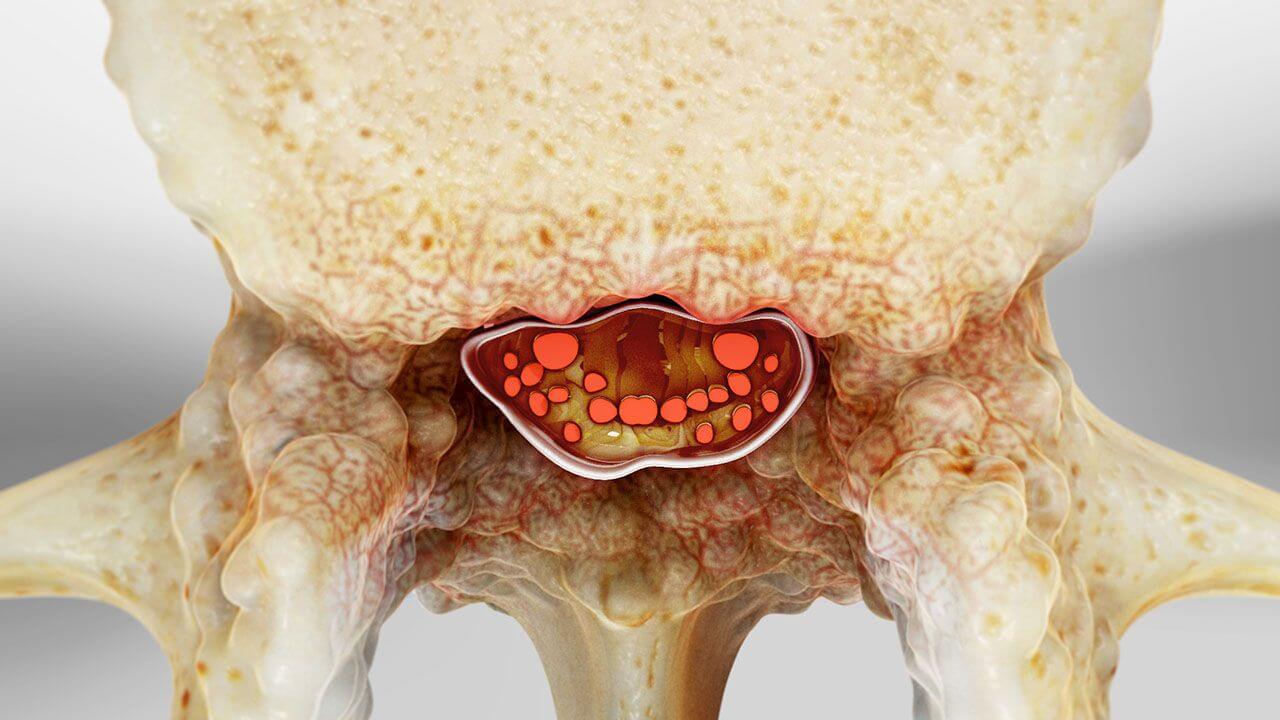
An HD endoscope with an attached HD camera is inserted into the cannula or often called a tubular retractor. The surgeon can now visualize on an HD monitor the spinal canal, vertebral disc and exiting nerves. Endoscopic spine surgery can treat effectively herniated disc, bulging disc and foraminal stenosis.
This ultra minimally invasive spine surgery is the most effective surgical technique that relieves a herniated disc, low back pain, and sciatica. Because it utilizes a 1/4 inch incision, patients recover faster than minimally invasive spine surgery.
This endoscopic spine surgery effectively treats painful conditions caused by a herniated disc, spinal stenosis, sciatica, and facet joint syndrome. This procedure is an excellent solution for patients suffering from pain seeking a faster return to an active lifestyle.
Minimally invasive spine surgery (MIS), the standard of care in spine surgery, represents a broad spectrum of techniques, with endoscopic being the least invasive. Endoscopic spine surgery is as effective as the MIS microdiscectomy procedure at relieving painful spine conditions.
However, unlike MIS, endoscopic spine surgery significantly reduces trauma to the patient’s muscles and soft tissue leading to faster recovery. The endoscopic procedure utilizes a surgical approach that avoids the major stabilizing muscles of the lower back.
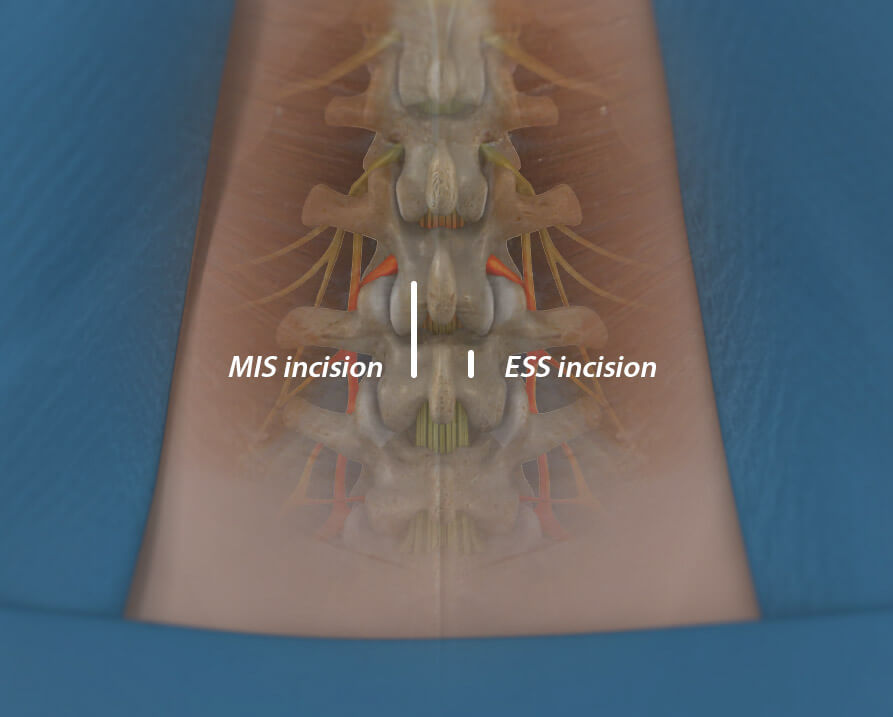
Unlike the MIS incision of one inch or more, ESS uses a ¼ inch incision. Smaller surgical incisions and avoiding major back muscles can significantly improve patient outcomes.
Sometimes called ultra-minimally invasive, the endoscopic spine surgery technique can be performed faster, allowing the surgeon better access to the spinal nerves and disc, and superior visualization. Also, ESS requires no general anesthesia, which affords patients less risk and faster discharge from the hospital within 2-3 hours of surgery.
Image for illustrative purposes only. Your physician will determine the actual incision placement.

Patients are lightly sedated with IV medication and positioned comfortably on the operating table. The surgeon then locally numbs the skin surgical site to ensure the patient is comfortable throughout the surgery.
Under fluoroscopic X-ray guidance, the physician guides a spinal needle and guidewire to the painful spinal disc. A micro-incision of ¼ inch is made. A metal dilator (the size of a pencil) and cannula are gently placed over the guidewire down to the spinal disc to establish the surgical portal. The guidewire and dilator are removed.
Specialized micro-instruments are placed through the endoscope to assist the surgeon in ablating and decompressing the affected spinal nerves. The surgeon often targets and resects herniated disc and bone spurs that may be impinging the spinal nerves.
Laser spine surgery is a marketing gimmick for many. Still, at DISC, our surgeons utilize a side-firing laser and radiofrequency energy often during ESS as one of many surgical instruments at their disposal.
After surgery, the spinal nerves are decompressed and free from impingement. A steroid injection is often administered thru the scope at the spinal level to enhance patient comfort and minimize post-operative inflammatory pain. The scope and cannula are removed, and one small stitch is used, applying a small bandage on the skin.
Patients are moved to recovery and monitored for an hour or two before being released to go home.
This is the most common least invasive procedure used to relieve the pressure of a herniated disc on a spinal nerve causing pain. It is also called Selective Endoscopic Discectomy, utilizing the world’s first working channel endoscope to perform direct visualized endoscopic spine surgery.
Endoscopic Facet Medial Branch Nerve Transection is an ultra-minimally invasive endoscopic procedure treating chronic low back pain caused by facet joints in your back. This procedure has been shown to provide up to five years of long-term relief. If you had short-term relief from a pain management radiofrequency ablation procedure, you might be a candidate.
This is an ultra-minimally invasive endoscopic laser spine surgery that targets foraminal stenosis, also called lateral recess stenosis. Lateral recess stenosis can be the cause of failed back surgery in up to thirty percent of patients. The endoscopic technique utilizes motorized burrs and a side-firing laser to enlarge the narrow boney foramen, thus relieving the exiting spinal nerve’s pressure. Endoscopic Foraminoplasty may help select patients avoid a minimally invasive spinal fusion.

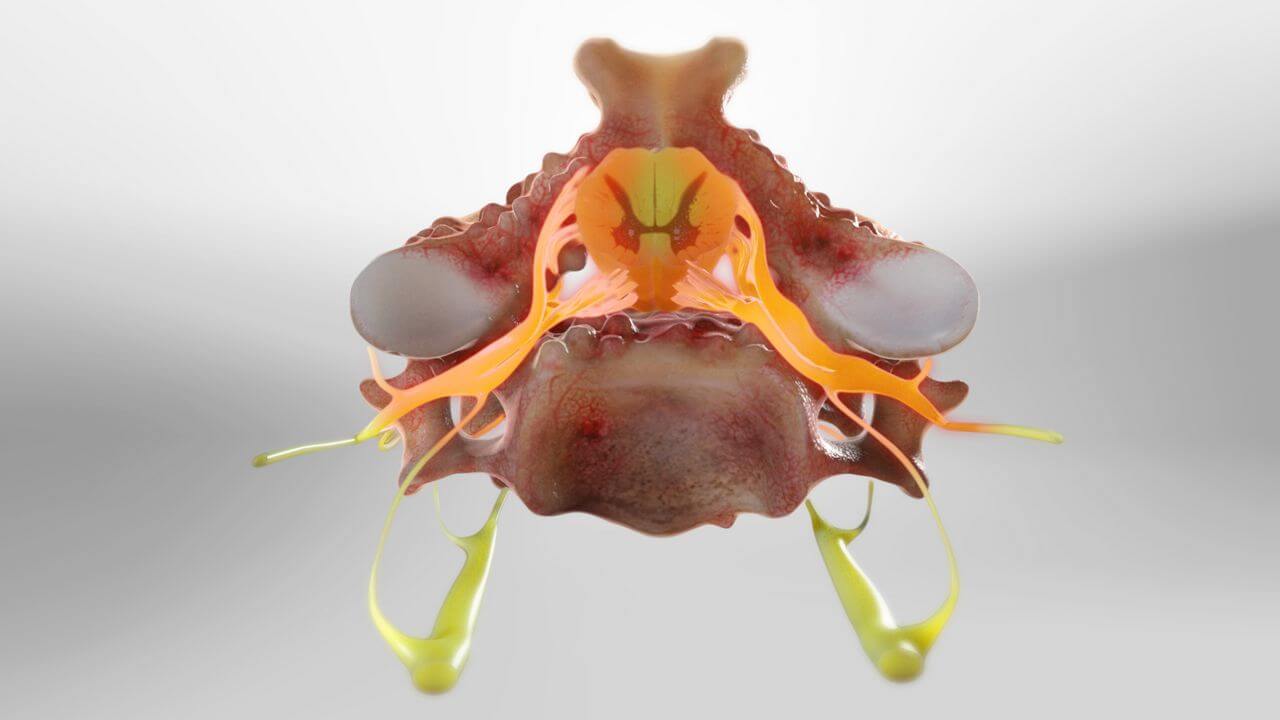
Traditional or minimally invasive spine surgery aims to improve pain by decompressing or relieving pressure and irritation on the spinal cord and exiting nerve roots. During spine surgery, a surgeon is cautious to preserve spinal anatomy and the functionality of the spinal muscles in the patient’s back.
Sometimes, a surgeon’s outcomes do not align with patient expectations. Although the surgery has been successful, patients often experience residual pain or pain from surgical disruption of the spinal anatomy and back muscles.

Endoscopic spine surgery is the least invasive surgical option for patients suffering from back and leg pain. Endoscopic spine surgery treats multiple painful spinal conditions such as:
The ideal candidate for endoscopic spine surgery can vary depending on the specific condition being treated and the surgeon’s assessment. However, in general, the following characteristics may make a patient a good candidate for endoscopic spine surgery:
Our candidate selection process begins with our proprietary Personalized Pain Mapping. Personalized pain mapping of the spine, also known as diagnostic spinal mapping, is a procedure performed to identify and locate the source of a patient’s chronic or persistent spinal pain. It is a diagnostic tool used by spine specialists to gain a better understanding of the specific areas causing pain in an individual patient.
We listen carefully to your pain journey and your desired outcomes. Then we use diagnostic and therapeutic injections to pinpoint the pain generator. We personalize a treatment plan that will effectively address your pain and desired outcomes. Many of our patients get better without any surgical intervention. However, those patients we select for endoscopic spine surgery have great results and a high level of satisfaction.
Personalize pain mapping of the spine allows for a more accurate diagnosis and helps our expert spine specialist tailor the least invasive and most effective treatment options for patients.
You may be a candidate for endoscopic spine surgery if you:
Due to evolving physicians’ treatment methodology, certain degenerative conditions, if not too severe, can be helped, but only after individual evaluation of each patient and their response to evocative discography and other diagnostic injections can our surgeons tell if the endoscopic procedure is recommended for you.
Make an Appointment
If you are seeking a second opinion or looking to travel for a less invasive surgery, our orthopedic spine specialists in Phoenix are available to help you get an accurate spine diagnosis and customize an innovative treatment plan to get back to enjoying life. Schedule an appointment with one of our compassionate expert spine surgeons today.
Our spine health blog features up-to-date spine education and expert spine tips from our spine specialists here at DISC.
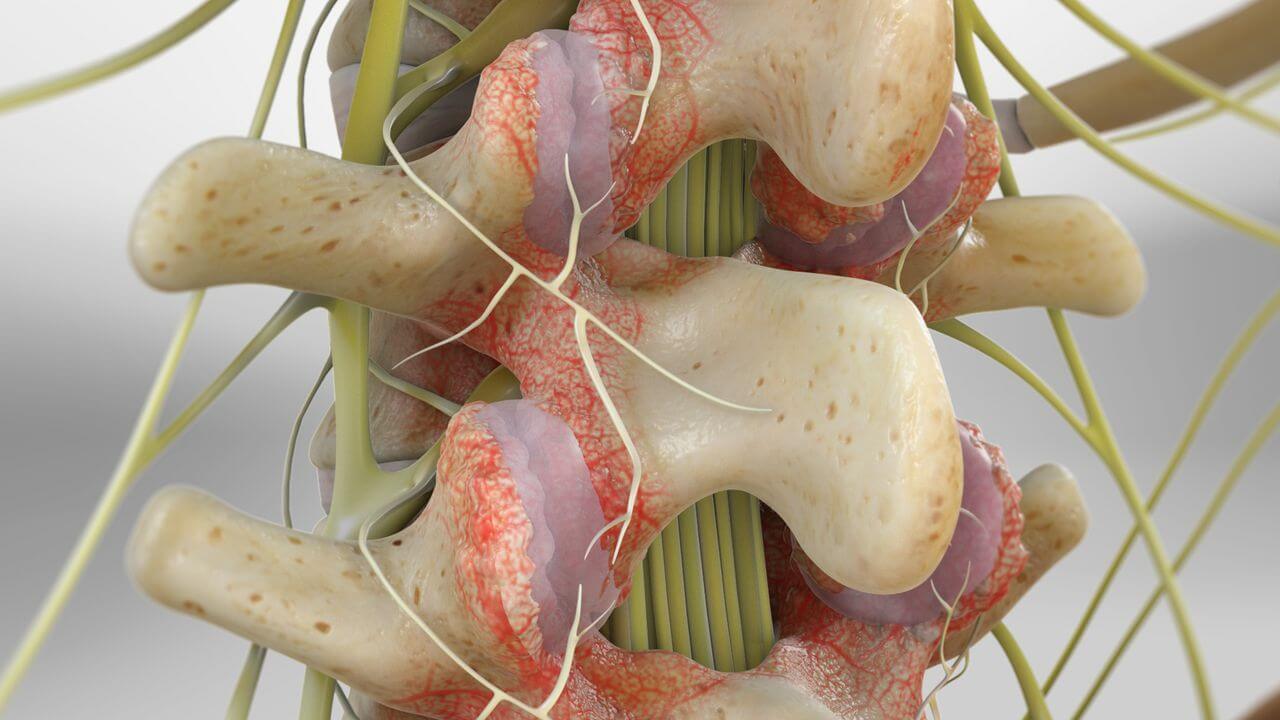
A pinched nerve, also known as radiculopathy in medical terms, is a condition in which one or more nerves are compressed or “pinched” and unable to function properly. This happens when the nerve suffers from too much pressure caused by surrounding tissues, such as bones, muscles, cartilage and tendons. Nerves function like electrical cables, transmitting signals between the brain, spinal cord and the rest […]
Any surgery can be intimidating, especially if you haven’t undergone one before. It’s natural to have questions about the process, including before-and-after care, to ensure a smooth process. Asking questions about your surgery can help prepare you for the event and provide peace of mind. Below are questions you may want to ask your surgeon […]
Are you tired of dealing with nagging back pain that radiates down your leg? You may be experiencing sciatica — a common but complex condition affecting the sciatic nerve, often leading to sharp, shooting pain from the lower back down to the legs.

If you’re reading this, chances are you’ve been living with chronic neck pain, perhaps caused by conditions like degenerative disc disease, herniated discs or cervical radiculopathy. The discomfort can range from mild annoyance to debilitating pain, affecting everything from your ability to work to your quality of life. But you’re here because you’ve […]

Are you considering or have recently undergone a cervical artificial disc replacement? If so, you’re on the path to relief. Chronic neck pain caused by degenerative disc disease or herniated discs can be debilitating. This advanced procedure removes and replaces a damaged disc with a prosthetic one. It preserves and restores neck motion. The result […]




Congratulations to DISC’s surgeons, Christopher Yeung, Justin Field, and Nima Salari, for being chosen as Phoenix Magazine’s TOP DOCTOR in 2023.
Register today for Amplify Surgical’s 2nd Annual Endoscopic Spine Symposium, featuring dualPortal™ and dualX® System on March 4, 2023.
Congratulations to Dr. Yeung for being featured on the front cover of Maricopa County Medical Society’s “Arizona Physician” Winter 2022 magazine!

Dr. Chris Yeung was interviewed by Arizona Physician Magazine – a publication that provides information for physicians across Arizona.

Dr. Salari received the most votes in the Orthopedic Surgery of the Spine category. Dr. Yeung received the award for the 10th consecutive year.
1635 East Myrtle Avenue Suite 100, Phoenix, AZ 85020, USA
18700 North 64th Drive Suite 105, Glendale, AZ 85308, USA
8630 East Vía de Ventura Suite 210, Scottsdale, AZ 85258, USA
3487 South Mercy Road, Gilbert, AZ 85297, USA
1635 East Myrtle Avenue Suite 400, Phoenix, AZ 85020, USA