Endoscopic Medial Branch Transection Procedure in Arizona
Endoscopic Medial Branch Transection Procedure in Arizona
An endoscopic rhizotomy or medial branch nerve transection, offered by DISC surgeons in Phoenix, AZ, is the least invasive yet most effective treatment option for chronic low back pain.
The outpatient procedure, performed through an ¼ inch incision, is the smallest in spine surgery. The endoscopic procedure targets the painful medial branch nerves located around the lumbar facet joints that relay the pain signal in your low back muscles to your brain.
When our surgeons directly visualize these nerves with an HD endoscope, they can ablate or transect the nerve using a laser or radiofrequency probe with confidence, thus providing patients with long-term pain relief.
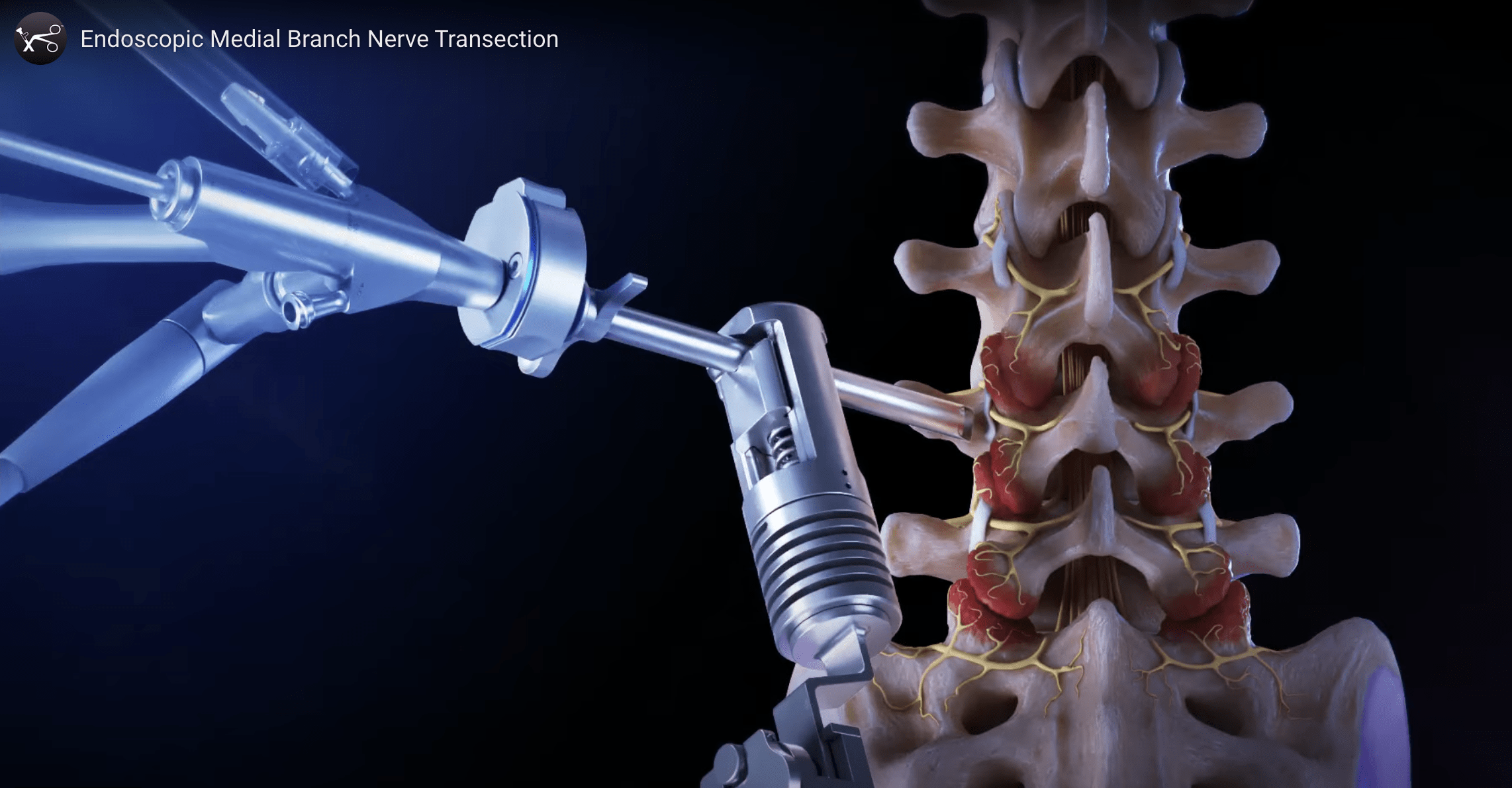
Endoscopic Medial Branch Nerve Transection
Endoscopic medial branch nerve transection is a ultra-minimally invasive procedure used to alleviate chronic back pain associated with facet joints in the spine. During the procedure, a small endoscope is guided to the affected area, allowing precise visualization of the medial branch nerves that transmit pain signals from the facet joints. By selectively severing these nerves, often using radiofrequency ablation or other thermal techniques, pain signals are interrupted, providing long-term relief to patients suffering from conditions like facet joint arthritis or spinal stenosis. This approach minimizes tissue disruption and recovery time compared to traditional surgery, making it a preferred option for those seeking effective pain management with fewer complications.
Video Credit: Arthrex
Invented & Developed at DISC
The endoscopic rhizotomy procedure was invented and developed at DISC by Anthony Yeung, MD (retired). Dr. Yeung saw a need to improve upon a pain management procedure called radiofrequency ablation (RFA), performed without direct visualization under X-ray guidance.
An RFA only provides patients temporary pain relief for six to twelve months. Endoscopic medial branch transection surgery significantly improves low back pain relief lasting up to five years. For many patients, this procedure is an excellent alternative to a lumbar spinal fusion. If you want to talk to one of our professionals about if an Endoscopic medial branch transection procedure is for you, contact us or make an appointment today!
What Symptoms Does an Endoscopic Medial Branch Transection Treat?
Endoscopic rhizotomy or medial branch nerve transection primarily treats symptoms associated with chronic back pain, particularly those arising from facet joint dysfunction. The symptoms it addresses include:
Chronic Low Back Pain: Persistent pain localized in the lower back, often related to facet joint arthritis or degeneration.
Neck Pain: Chronic pain in the cervical spine, typically due to facet joint issues.
Pain Radiating to the Buttocks or Thighs: Discomfort that spreads from the lower back to the buttocks or upper thighs, which can be indicative of facet joint problems.
Stiffness and Limited Range of Motion: Reduced flexibility and difficulty in bending or twisting the spine.
Pain with Movement: Increased pain during specific movements or activities, such as bending backward or twisting.
Tenderness over the Facet Joints: Sensitivity and pain when pressure is applied to the area over the facet joints.
These procedures are particularly beneficial for patients who have not found relief through conservative treatments such as medication, physical therapy, or injections.
What Conditions Can be Treated with an Endoscopic Rhizotomy?
Proper patient selection is crucial to the success rate of an endoscopic rhizotomy. At DISC, all patients undergo a personalized pain mapping process that selectively pinpoints the low back pain generator. Suppose patients get significant (greater than 50%) pain relief from a medial branch injection or facet joint injection. In that case, they typically respond very well to an endoscopic rhizotomy. Endoscopic medical branch nerve transection patients report a 90% success rate with up to 5 years of pain relief.
How is an Endoscopic Medial Branch Nerve Transection or Rhizotomy Performed?
An endoscopic rhizotomy is genuinely the least invasive outpatient surgery. Before the procedure, our anesthesiologist or trained nurse will place an intravenous (IV) catheter on your wrist and then take you to the operating room.
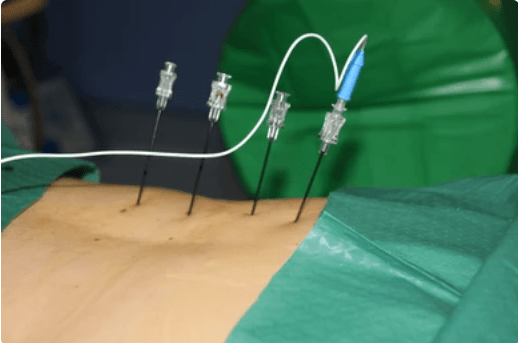
Once positioned on the table and comfortable, the anesthesiologist will administer conscious sedative medicine through your IV. Under X-ray, our surgeon will precisely target and mark your painful facet joints or transverse process. Then he injects a local anesthetic at the skin surgical site for your maximum comfort. I needle is placed under X-ray down to the transverse process bone where the medial branch nerve is located. A guidewire is placed inside the needle and needle removed. An 1/4 inch incision is made and a metal dilator is inserted over the guidewire through the incision gently dividing the muscles. Over the dilator a metal access cannula is placed on the transverse process bone and the dilator is removed. The surgeon now introduces an HD endoscope to visualize the medial branch nerves.
The surgeon utilizes a radiofrequency probe or straight firing laser to ablate and transect the medial branch nerve. Transecting this small nerve disconnects the pain signal from your back to your brain. Afterward, the cannula is removed from your back, and the incision is closed with a Steris strip band-aid.
The process is repeated for each painful nerve level on one or both sides of your back. The rhizotomy procedure only takes about 30-45 minutes on average.
Endoscopic Rhizotomy vs. Radiofrequency Ablation (RFA)
There are many differences between an radiofrequency ablation (RFA) and an endoscopic rhizotomy.
The endoscopic medial branch nerve transection technique is vastly more effective at providing
long-term back pain relief than a pulsed or continuous radiofrequency ablation. Both procedures
target the pain generator – medial branch nerve of the dorsal ramus, located around the facet
joints in your back.
The RFA procedure is done percutaneously under C-arm fluoroscopic X-ray and not directly
visualized with the physician’s eye. On the other hand, the endoscopic rhizotomy is directly
visualized by the surgeon with an endoscope and HD camera.
Dr. Abrams performing endoscopic medial branch transection
Percutaneous Radiofrequency Ablation
The dorsal ramus’s anatomy that innervates the facet joint varies and can contribute to pain management’s failed or
short-term results from the RFA procedure. The nerves can also entirely bypass the transverse process, and go
directly into the adjacent facet joint. The RFA procedure merely puts a lesion on the nerves through radiofrequency
energy. The nerves regenerate, and the pain returns within 6 – 12 months. The endoscopic rhizotomy is the most
effective method to ablate the branches of the dorsal ramus. The endoscopic procedure allows the surgeon to identify
the painful nerves, directly visualize and then ablate the nerves resulting in long-term relief up to 5 years.
DISC’s innovative surgery is also less invasive and less surgically morbid procedure than a spinal fusion. The
recovery for endoscopic rhizotomy is two weeks versus three months for a spinal fusion.
What are the Expected Recovery and Success Rates of an Endoscopic Medial Branch Transection?
After an endoscopic medial branch transeection, some patients may experience mild swelling, discomfort, and soreness around the skin incisions. These symptoms may linger for a few days up to a couple of weeks. Patients typically use over-the-counter pain relievers and an ice pack to provide relief.
Recovery
Most patients can return to work and normal activities the next day. However, they should avoid strenuous exercise and heavy lifting until advised by the surgeon. Taking a shower, soaking in the bathtub, or swimming should be avoided until at least 24 hours after surgery.
In our experience and our published research, patients who have an endoscopic rhizotomy can expect low back pain to be significantly improved post-operatively and continue to improve to maximum pain relief in about two weeks. This pain relief, as reported in clinical research, can last up to 5 years.
Success Rate
The success rate of endoscopic medial branch transection can vary depending on various factors, including the underlying cause of the pain, patient selection, and the skill of the surgeon performing the procedure. Generally, endoscopic rhizotomy has shown promising results in reducing or eliminating low back pain in selected patients who have not responded to conservative treatments.
Clinical studies have a reported success rate of 90% pain relief for a term up to 5 years following endoscopic rhizotomy.
When is an Endoscopic Medial Branch Transection Recommended?
Patients suffering from chronic low back pain related to the facet joints for more than six weeks should seek a second opinion before major spinal surgery.
Suppose you failed to get long-term relief from a pain management radiofrequency ablation (RFA) procedure. In that case, you might be a candidate for an endoscopic rhizotomy.
Some patients offered spinal fusion surgery for low back pain may benefit instead from an endoscopic Medial branch transection as a less invasive alternative.
Am I a Candidate?
You may be a candidate for endoscopic rhizotomy if you:
Low back pain for more than six weeks
Low back palpation by surgeon contributes to pain or spasm
Greater than 50 percent relief from medial branch nerve block or facet joint injection
Symptoms and pain return after a radiofrequency ablation
If, after reading the above, you believe endoscopic rhizotomy may help you, feel free to contact us for an appointment. Out-of-state and interested in a second opinion? Please fill out our consult request form and a member of the DISC staff will reach out to you immediately.
No matter the painful spine condition, a second opinion consultation with one of our expert spine surgeons can help you find the right customized solution that gets you back to enjoying life.