
- Bryan Cervical Disc
- M6-C *
- Mobi-C *
- PCM Cervical Disc System
- ProDisc-C *
- Secure-C
- Simplify Disc
In short and long-term clinical studies, the success rates for cervical artificial disc replacement surgery are superior to the anterior cervical discectomy and fusion surgery.
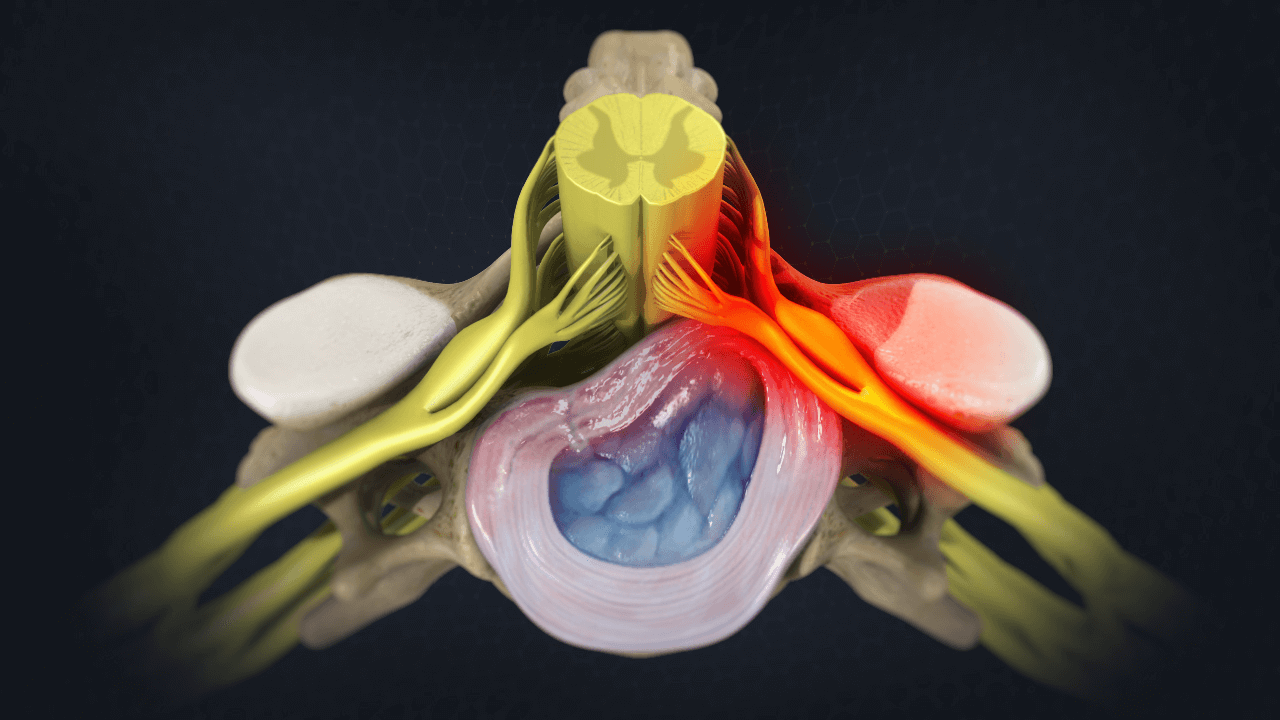
Cervical artificial disc replacement has undergone rigorous clinical studies, resulting in an effective and safe treatment option for cervical disc degeneration with myelopathy or radicular symptoms.
In short and long-term clinical studies, the patient satisfaction and clinical success rates for artificial cervical disc (CDR) replacement surgery are equal at one-level surgery and superior at two-level surgery to the anterior cervical discectomy and fusion surgery (ACDF). Greater than 95% of patients who underwent CDR and 88% of patients who underwent ACDF were “very satisfied” at seven years.
The potential patient benefits of artificial disc replacement versus spinal fusion surgery may include:
The key to success with cervical artificial disc replacement is proper patient selection. Not all patients are candidates for disc replacement. Patients with severe degeneration, spinal instability, and significant osteoporosis are contraindicated for CDR. They may be better selected for ACDF surgery.

“In our clinical experience, ideal candidate patients undergoing cervical ADR have a faster return to activity, greater satisfaction, and lower rates of need for additional surgery.”
– Board-Certified Orthopedic Spine Surgeon Dr. Nima Salari
Artificial disc replacement (ADR) is a motion preservation spine surgery that removes a painful damaged spinal disc and replaces it with an artificial disc. This surgery is performed in the low back or the neck.
Cervical artificial disc replacement surgery is performed by a spine surgeon with the
patient under anesthesia.
While the patient is asleep lying on their back, the spine surgeon will make a one-to-two-inch
incision on the front of your neck. The surgeon then removes the affected cervical disc and replaces it with an artificial disc.
The surgery lasts about 1-2 hours as an outpatient minimally invasive procedure with patients going home a few hours after surgery.
While the patient is asleep lying on their back, a vascular surgeon assisting the spine surgeon will make a 2-inch incision in the abdomen. The muscle is gently retracted as are the deeper structures including the peritoneal sac and the major blood vessels are moved to the side to create access to the affected lumbar disc. The spine surgeon then removes the damaged degenerative disc and replaces it with an artificial disc. The patient is moved to recovery. The surgery lasts about 2-3 hours as an outpatient minimally invasive surgery. Most patients go home after a short recovery in the hospital.
Cervical artificial disc replacement surgery will restore your mobility to what it was before surgery. Removing and replacing the painful degenerative disc will relieve the spinal nerves’ pressure, eliminate pain, numbness, and tingling, and significantly improve your quality of life.
After surgery, you should have some pain and discomfort as with any surgery. Patients are discharged from the hospital in a few hours. Your surgeon will provide you with medication to control pain and specific guidelines for return to work and activities when leaving the hospital. Unlike spine fusion surgery, a cervical brace is not usually recommended. Most patients return to work and normal activities between two and six weeks.
As with any surgery, cervical spine surgery has potential risks and complications. There is always the risk for anesthesia complications, allergic reactions, and blood clotting with any spine surgery due to undiagnosed medical conditions such as those related to heart disease.
Potential risks and complications related to any cervical artificial disc replacement surgery may include:
|
|

Although the ADR devices have only been approved and implanted since 2000, five and ten years post-operative outcome studies look very promising. According to many of the manufacturers of these devices, they should last about 40 years.
Unlike a spinal fusion that limits motion by fusing two adjacent vertebrae, the artificial disc replacement preserves motion like a healthy spinal disc. In fact, in recent studies of ADR versus spinal fusion, patients who had ADR surgery were less likely to have needed additional surgery in the future. For this reason and many more, ADR has become the preferred surgery by many expert spine surgeons to treat degenerative disc disease.
Many of the major insurance carriers cover artificial disc replacement (ADR) based on risks, benefits, and cost of the procedure. However, if your insurance covers ADR, your specific health plan may have restrictions on which patients are approved.
Many insurers still consider cervical disc replacement surgery for degenerative disc disease investigational and experimental and therefore do not cover it. At DISC, our expert spine surgeons are significant advocates of cervical ADR. They often recommend this surgery for suitable candidates.
The limits vary from plan to plan but usually include the following to receive approval:
If you are a candidate, our insurance experts will assist you in getting the surgery approved.
Some health insurance carriers will deny a doctor’s recommendation for a lumbar or cervical artificial disc replacement. Each plan has restrictions on which patients are candidates for approval. When a patient has exhausted all internal and external appeals, they are left with two alternatives. Live with chronic back or neck pain or pay out-of-pocket for spine surgery. If you consider the out-of-pocket expenses, it is essential to understand all of the costs associated with the surgery before moving forward with your surgeon.
The total cost of disc replacement surgery can include the spine surgeon, the anesthesiologist, the vascular surgeon (lumbar surgery), the implant, and the facility’s fees. These fees can be bundled into one or two bills. Make sure to clarify the cost and billing with the surgeon’s office. The total cost of an artificial disc replacement surgery can range from $25,000 to $70,000, with cervical surgery on the lower end and lumbar on the upper end of the price range.
Other costs associated with artificial disc replacement will be pre-operative clearance, including evaluation, bloodwork, X-ray, MRI, and ECG studies. Post-operative, you may need physical therapy or rehabilitation. If paying out-of-pocket, this cost can be charged against your deductible.


Over the past 30 years, there have been a variety of artificial disc replacement devices investigated as an alternative to spinal fusion. This surgical solution is also called spinal arthroplasty or total disc replacement.
The goal of the device is to maintain motion at the surgical level once the damaged disc has been removed and maintain normal biomechanics of the adjacent vertebrae levels above and below the new ADR.
The short answer is yes.
“An artificial disc replacement device may be replaced depending on the presenting symptoms and cause for consideration of the replacement. First, if the device has failed, but the segment is not too arthritic, you could consider a different device. Second, the failed device can be converted to a spinal fusion.” – Dr. Nima Salari
“You can exercise within a week of cervical artificial disc surgery. You want to limit high-intensity activity immediately after surgery to avoid increasing blood pressure, heart rate, and risk of bleeding. Otherwise, the patient can return to regular activities within a week with a gradual return to heavy exercise.” – Dr. Nima Salari
“One can return to exercise around the second month after lumbar artificial disc replacement surgery due to healing of the abdomen from the surgical approach.” – Dr. Nima Salari
“Yes. Artificial discs can be implanted at multiple levels in the neck. The FDA has approved select disc replacements for two consecutive levels from C3-C7 in the cervical spine.
You may consider additional levels, but there are limited studies, and off-label use of the product is up to the discretion of the spine surgeon in charge of your care.” – Dr. Nima Salari
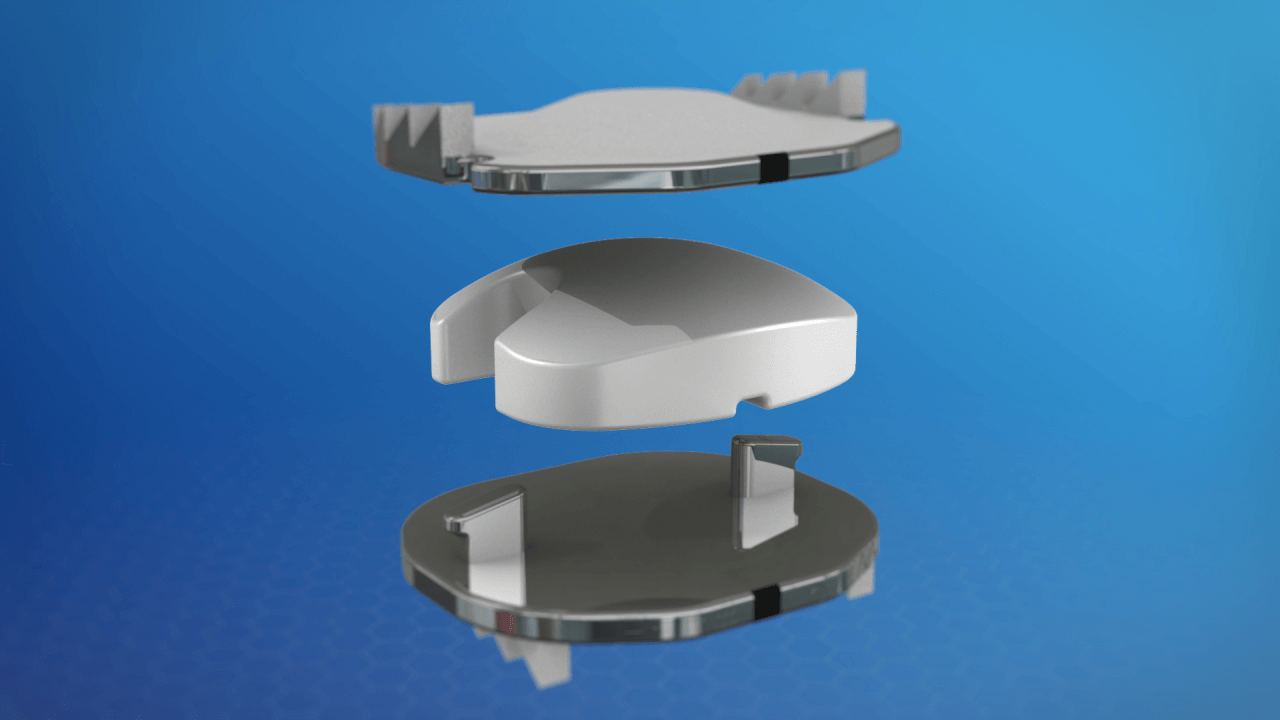
“Each of the approved artificial disc replacement devices is unique and has many different features. No one device is always the best fit for all patients. We encourage all patients to learn about each device, its makeup, and mechanisms which vary slightly.
Our goal here is not to promote one device over the other. The most common materials used are metal endplates with a polymer like a knee and hip replacement in the middle.” – Dr. Nima Salari
DISC offers a complete range of nonsurgical, ultra-minimally invasive, motion-preserving, and minimally invasive solutions for patients suffering from painful neck and back conditions.
Our spine health blog features up-to-date spine education and expert spine tips from our spine specialists here at DISC.
A pinched nerve, also known as radiculopathy in medical terms, is a condition in which one or more nerves are compressed or “pinched” and unable to function properly. This happens when the nerve suffers from too much pressure caused by surrounding tissues, such as bones, muscles, cartilage and tendons. Nerves function like electrical cables, transmitting signals between the brain, spinal cord and the rest […]
Any surgery can be intimidating, especially if you haven’t undergone one before. It’s natural to have questions about the process, including before-and-after care, to ensure a smooth process. Asking questions about your surgery can help prepare you for the event and provide peace of mind. Below are questions you may want to ask your surgeon […]
Are you tired of dealing with nagging back pain that radiates down your leg? You may be experiencing sciatica — a common but complex condition affecting the sciatic nerve, often leading to sharp, shooting pain from the lower back down to the legs.

If you’re reading this, chances are you’ve been living with chronic neck pain, perhaps caused by conditions like degenerative disc disease, herniated discs or cervical radiculopathy. The discomfort can range from mild annoyance to debilitating pain, affecting everything from your ability to work to your quality of life. But you’re here because you’ve […]

Are you considering or have recently undergone a cervical artificial disc replacement? If so, you’re on the path to relief. Chronic neck pain caused by degenerative disc disease or herniated discs can be debilitating. This advanced procedure removes and replaces a damaged disc with a prosthetic one. It preserves and restores neck motion. The result […]



Congratulations to DISC’s surgeons, Christopher Yeung, Justin Field, and Nima Salari, for being chosen as Phoenix Magazine’s TOP DOCTOR in 2023.
Register today for Amplify Surgical’s 2nd Annual Endoscopic Spine Symposium, featuring dualPortal™ and dualX® System on March 4, 2023.
Congratulations to Dr. Yeung for being featured on the front cover of Maricopa County Medical Society’s “Arizona Physician” Winter 2022 magazine!

Dr. Chris Yeung was interviewed by Arizona Physician Magazine – a publication that provides information for physicians across Arizona.

Dr. Salari received the most votes in the Orthopedic Surgery of the Spine category. Dr. Yeung received the award for the 10th consecutive year.
1635 East Myrtle Avenue Suite 100, Phoenix, AZ 85020, USA
18700 North 64th Drive Suite 105, Glendale, AZ 85308, USA
8630 East Vía de Ventura Suite 210, Scottsdale, AZ 85258, USA
3487 South Mercy Road, Gilbert, AZ 85297, USA
1635 East Myrtle Avenue Suite 400, Phoenix, AZ 85020, USA