If you’ve been told you need open back surgery or spinal fusion, you have options. Endoscopic decompression is a minimally invasive procedure that relieves nerve pressure without large incisions, extensive muscle damage or the need for hardware like screws and rods. Endoscopic spine surgery offers patients a path to relief that preserves spinal stability and helps get them back to their lives faster.
If you are dealing with sciatica, spinal stenosis or a herniated disc, endoscopic spinal decompression targets the source of your pain while leaving healthy tissue intact. Many patients walk out the same day and return to limited activities in weeks, not months.
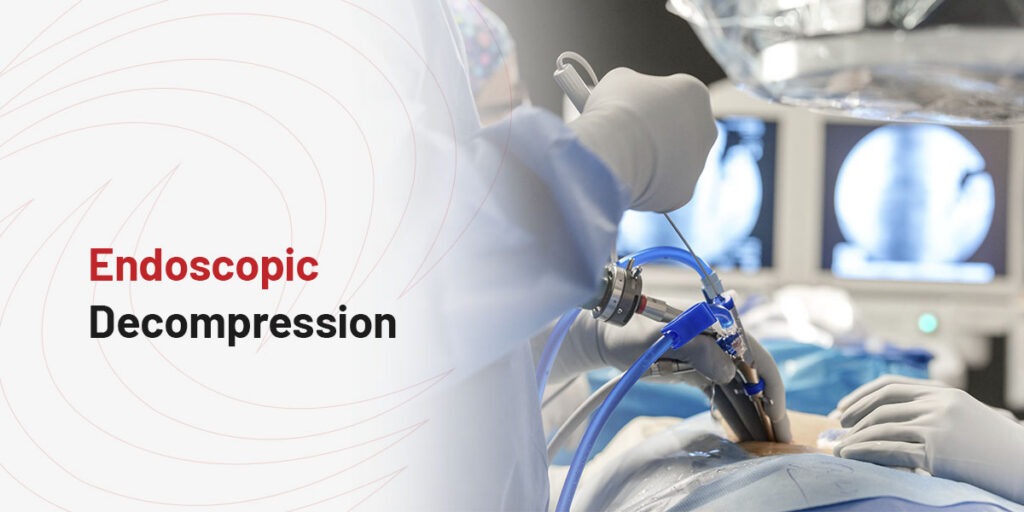
The targeted surgical technique relieves pressure on compressed spinal nerves using an endoscope — a thin tube with a camera and light. Unlike traditional open surgery, this approach doesn’t need large incisions or cutting through muscle layers. The goal is to remove only the tissue causing nerve compression, like herniated disc material, bone spurs or thickened ligaments, while preserving the spine’s natural stability.
The procedure starts with a small incision, typically less than one-quarter inch. The surgeon inserts a narrow cannula to create a working channel to the affected area. An endoscope is guided through this channel, providing direct visualization of the compressed nerve. The surgeon removes only the material pressing on the nerve.
Research supports the benefits of this approach. A systematic review found that endoscopic spine surgery, compared to traditional open surgery, offers:
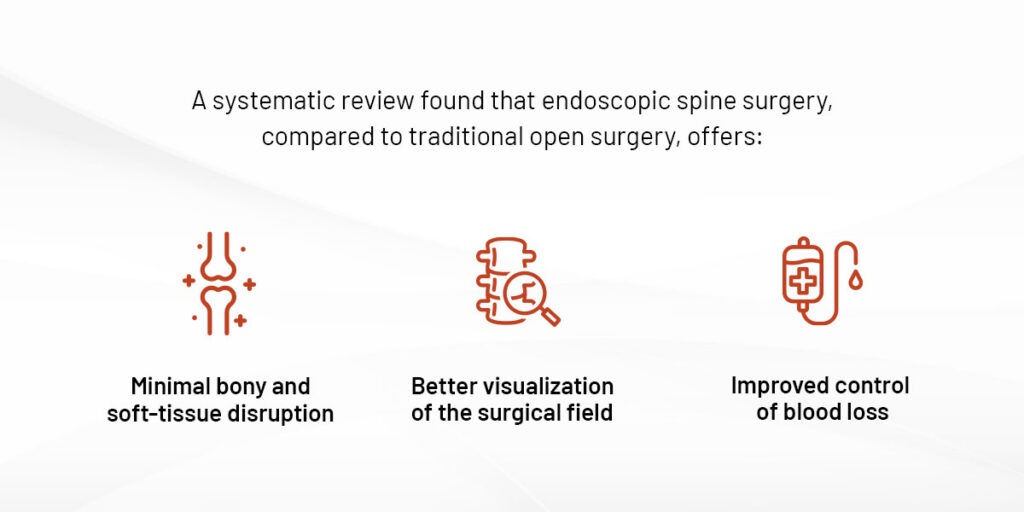
These advantages translate to shorter hospital stays and faster functional recovery for patients.
Traditional decompression techniques such as laminectomy relieve pressure on the nerves by decompressing lamina and ligaments and preserves spinal stability. Spine fusion with screws, rods and bone graft are usually used with pre-existing instability, severe spinal stenosis or degenerative disc disease.
Endoscopic decompression keeps the structural integrity of the spine intact by removing only what’s compressing the nerve. Endoscopic techniques show better muscle preservation and similar decompression success compared to open laminectomy. By maintaining the facet joints and ligaments, the spine remains more stable, often eliminating the need for fusion.
Understanding your surgical options helps you make an informed decision. Laminectomy removes part or all of the lamina — the back part of the vertebra — to create more space for compressed nerves. Fusion uses screws, rods and bone grafts to permanently join two or more vertebrae together, eliminating motion between them.
Here’s how endoscopic decompression spine surgery procedure compares to traditional laminectomy and spinal fusion.
The size of the incision and how surgeons access the spine affect tissue trauma and recovery:
Endoscopic decompression: The procedure uses an incision of less than one inch. Muscle fibers are gently spread, leaving them intact and functional.
Laminectomy: This requires a 1 to 2-inch incision depending on how many spinal levels need decompression. Surgeons often cut and spread the muscle with retractors to reach the spine, which causes postoperative pain and longer healing.
Fusion: A larger incision of 2 to 3 inches or more is needed. Extensive muscle cutting is necessary to place hardware.
Recovery expectations vary significantly depending on the surgical approach:
Endoscopic decompression: Most patients go home the same day. Many return to desk work within 1 week and resume limited physical activities within 3 to 4 weeks.
Laminectomy: A 1 day hospital stay is sometimes required. Recovery takes 4 to 6 weeks before returning to limited activities.
Fusion: Patients usually have a 1 to 2 days hospital stay. Full recovery can take 4 to 6 months, with significant activity restrictions during the healing process.
Whether your spine maintains its natural flexibility depends on the procedure performed:
Endoscopic decompression: The facet joints and ligaments are preserved, maintaining natural spine movement. This approach is effective even for complicated cases without needing fusion.
Laminectomy: The procedure may preserve motion if the facet joints remain intact, but removing too much bone can lead to instability that requires fusion.
Fusion: Motion is permanently eliminated between fused vertebrae. This can increase stress on adjacent spine segments over time.
The degree of tissue disruption directly correlates with pain levels after surgery:
Endoscopic decompression: Studies suggest that patients experienced significantly less back pain after surgery due to muscle preservation.
Laminectomy: Muscle trauma can lead to moderate to significant postoperative pain, which typically decreases over several weeks.
Fusion: Substantial postoperative pain can occur from the incision and hardware placement. Pain management is more intensive and prolonged.
Guided by your surgeon, the right approach depends on your specific spinal condition and stability. Endoscopic decompression is generally best for herniated discs, spinal stenosis and foraminal stenosis where the spine is stable or can remain stable after decompression.
Laminectomy may be used when larger areas of bone need removal to decompress nerves, but the spine will remain stable afterward. Fusion is often necessary when the spine is already unstable, has significant deformity, or when decompression alone would create instability. It is also used for conditions like spondylolisthesis with slippage.
The minimally invasive surgery treats several conditions that cause nerve compression and radiating pain.
Spinal stenosis is a narrowing of the spinal canal that puts pressure on the spinal cord or nerves. This narrowing often results from thickened ligaments, bone spurs or bulging discs. Endoscopic surgery removes the tissue and bone causing the narrowing while preserving the structural elements that keep the spine stable.
When disc material protrudes from its normal position and presses on a nerve root, it can cause pain that often radiates down the leg. Endoscopic spinal decompression allows surgeons to remove the herniated fragment. The procedure accesses the disc through a small portal, removes only the portion causing compression and leaves the rest of the disc intact.
Foraminal stenosis happens when the opening through which nerve roots exit the spine narrows. This compression, often characterized by sharp pain shooting down the leg, is one of the causes of sciatica. Traditional surgery sometimes misses foraminal narrowing because the approach doesn’t provide good access to this area. Often traditional surgery for foraminal stenosis can lead to failed back surgery syndrome.
Endoscopic surgery for spine decompression excels at treating foraminal stenosis. The endoscope can be positioned to directly visualize and treat the compressed nerve in the foramen. Endoscopic foraminoplasty enlarges the foramen by removing bone spurs and tissue, creating more room for the nerve.
Surgery is typically considered after nonsurgical treatments haven’t provided adequate relief. If you’ve tried these approaches for several weeks or months without significant improvement, you may be a good candidate for endoscopic spinal decompression. Progressive weakness, severe pain that limits daily activities, or worsening numbness are signs that surgery might be needed.
If spinal fusion has been recommended, it’s worth getting a second opinion. Not all nerve compression needs fusion. In many cases, endoscopic decompression provides relief without the need for hardware.
The techniques used today were developed and refined by DISC, making us among the pioneers of endoscopic spine surgery.
The founder of DISC, Dr. Anthony Yeung, developed the first FDA-cleared endoscopic spine system — the Yeung Endoscopic Spine System (YESS™). This groundbreaking work laid the foundation for modern endoscopic spinal decompression and created an entirely new subspecialty, Surgical Pain Management. When you choose DISC, you’re working with surgeons who helped develop these procedures and have trained spine specialists worldwide.
You don’t have to settle for open surgery or live with chronic pain. DISC’s surgeons specialize in treating the pain generator without destabilizing your spine. If you’ve been told you need fusion or conservative treatments haven’t worked, a second opinion can make all the difference.
Contact DISC today to schedule a consultation and find out whether endoscopic decompression can help restore your lifestyle and help you enjoy life again.
Linked Sources: